May 9, 2023
Blepharoptosis is one of the most common eyelid conditions. More than 13 million people in the U.S. have low-lying eyelids or blepharoptosis. Approximately one in ten people older than 50 have blepharoptosis as the incidence rate does increase with age.
If you are looking for an opportunity to get into aesthetics, start with the lids. But first, you’ll need to learn what causes blepharoptosis, how to identify it, and why ECPs have the solutions to offer patients. It’s also important to discuss these facts with your patients.
First, the key to aesthetics is to get out from behind the slit lamp. A proper assessment of the patient consists of conversation and astute observation.
Start with the Lids
First, what causes acquired blepharoptosis? Remember there are two muscles that elevate the lid: the levator muscle and Müller’s muscle. The levator muscle is innervated by CN III, controls lid opening, transitions from muscle to an aponeurosis, and where it inserts into the anterior tarsal plate forms the upper eyelid crease. Müller’s muscle originates from and works with the levator muscle. It inserts into the superior tarsal plate, is sympathetically innervated, regulates the palpebral fissure width, and is responsible for elevating the lid about 2 mm.
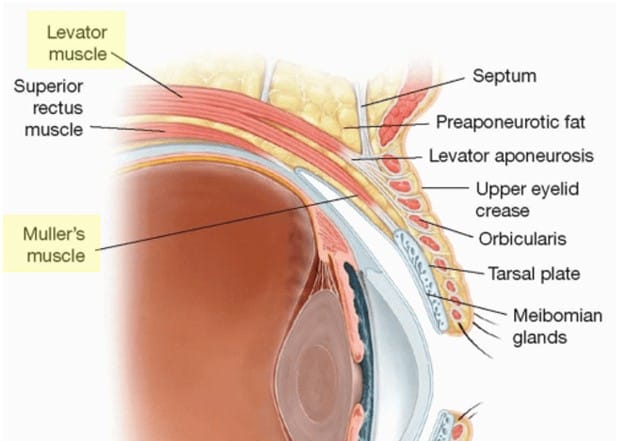
Figure 1. Identifying Müller’s muscle, the levator muscle, and levator aponeurosis insertion which forms the lid crease
The most common cause of acquired blepharoptosis is the result of stretching, dehiscence, or disinsertion of the levator muscle complex that occurs with the aging process. Other causes include neurogenic mechanisms or reduced input from the nerve responsible for innervation. Trauma can cause an injury either to the muscle or the nerve. Mechanical causes, such as eyelid heaviness from dermatochalasis or eyelash extensions, can also be responsible. Remember, blepharoptosis can be a sign of a much bigger disease state going on such as Horner syndrome, CNIII palsy, Myasthenia gravis, or chronic progressive external ophthalmoplegia (CPEO).
Here are some questions to ask when you see blepharoptosis: Is it unilateral? New onset? Pupil involvement? Double vision? Is levator dehiscence present? If the answer is yes to any of these questions, then the patient needs a full workup by you to determine the cause. In this article, we are focused on the benign acquired blepharoptosis that comes with age.
Identifying patients with blepharoptosis can be very simple. Here are all the ways to easily identify an issue with eyelids. First, the marginal reflex distance (MRD-1) is great way to look for the twinkle in a patients’ eye. While it can be measured with a PD ruler, I prefer to look at the anatomy during the patient assessment. Utilizing a transilluminator, you are simply looking for the reflection from the patient’s pupil center and the distance to the upper lid margin.
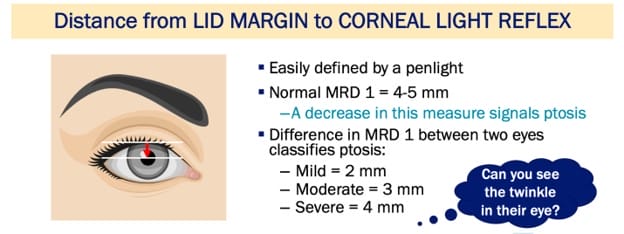
Figure 2. Depicting MRD-1 measurement
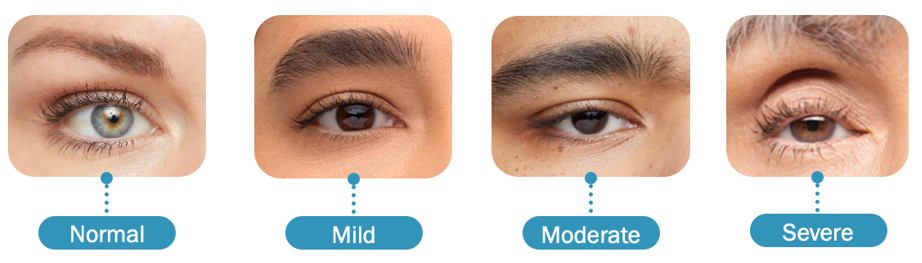
Figure 3. Showing range of MRD-1 from normal to severe
Another way to look at the lids is to notice or measure the distance between the lid margin and the lid crease, this is the lid platform or tarsal plate show (TPS). Attractive eyes exhibit less TPS,1 and increased TPS has been associated with higher perceived age, tiredness, and sadness.2
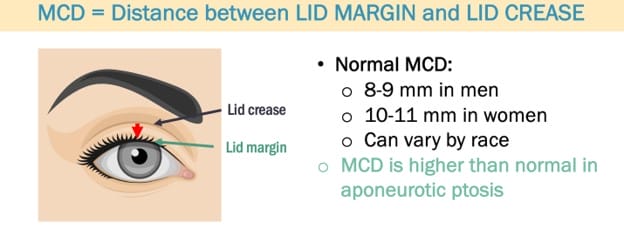
Figure 4. Depicting TPS measurement

Figure 5. Showing small lid platform to large lid platform
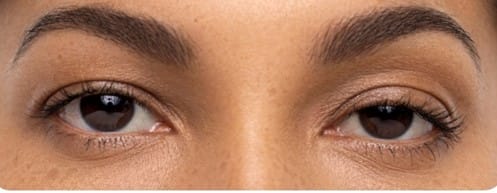
Another measurement is looking at the upper eyelid height (UEH). This is the distance between the lower brow border to the center of the lid margin. Attractive eyes exhibit lower UEH. Neuromodulator injections that lift the brow increase UEH, often creating an undesirable look. Lifting the upper eyelid decreases UEH, which makes eyes more desirable.3
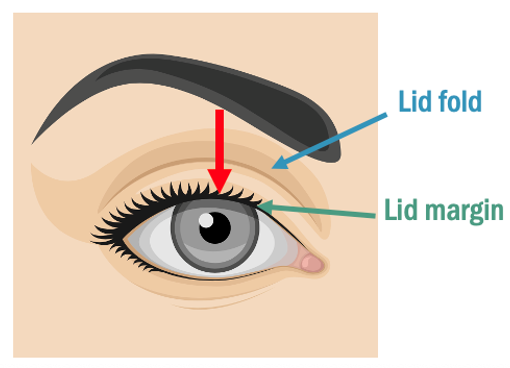 Figure 6. Demonstrating UEH
Figure 6. Demonstrating UEH
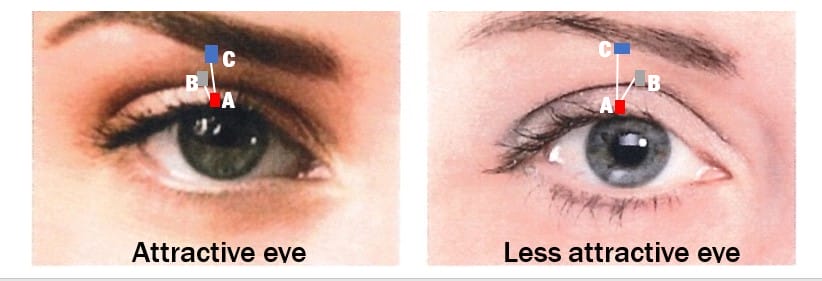
Figure 7. Demonstrating UEH
Three Simple Questions Make Lid Assessment Easy
1. What is the relationship between the pupil, iris, and upper lid margin? (MRD-1) Can you see the twinkle in the eye?
 2. Does one eye appear smaller than the other? Is there asymmetry?
2. Does one eye appear smaller than the other? Is there asymmetry?
3. How much lid platform is showing?

Eyes are the central feature of beauty, and ideal beauty is often a matter of millimeters.4 Studies show that eyes are the single most important facial feature with respect to perceived beauty.5 The eyes are the first to show signs of aging due to the delicate skin being thinner in the periorbital region. Are you comfortable identifying blepharoptosis?
Blepharoptosis Can Affect Patients’ Vision
Blepharoptosis isn’t only an aesthetic cosmetic concern. It can have a functional impact as well. How does blepharoptosis affect patients’ vision? Visual field impairment can occur when the MRD-1 is less than 4 mm. With an MRD-1 of 2 mm, the superior visual field impairment is in the range of 24-30%. That correlates to a whopping 12-15 degrees of visual field loss. This can impact patients in a variety of ways, even increasing fall risk.
What about the patient who is 20/20 unhappy? Meaning they have poor quality of vision even though they measure 20/20. Studies show that a low-lying lid increases higher order aberrations (HOA).4 Patients who underwent an upper lid blepharoplasty had increased contrast sensitivity, improved visual acuity, and significant changes in anterior corneal HOA reduction and changes in posterior corneal HOA. 4,5 All of this equates to improved visual quality. Many of our patients can benefit by having their eyelids lifted even 2 mm – patients with multifocal IOLs, AMD, cataracts, multifocal contact lens wearers. If their eyelid is causing reduced contrast, HOAs, and decreased vision, ODs can help!
What Can We Do About Blepharoptosis?
A non-invasive approach is to prescribe the drop 0.1 % oxymetazoline. I have found it works great in my clinic flow to have the patient instill it in their right eye during pre-testing so that by the time they are ready to be seen the drop is already working, which is about 15 minutes, as shown in Figure 8. This is a great way to have an educated discussion with the patient while in the office. I instill a drop in their left eye before they leave to balance them. Utilize this drop as your “gateway” drug into more in-depth aesthetics discussions.

Figure 8. Showing a patient 15 minutes after instilling I gt oxymetazoline 0.1%. Notice the “twinkle,” the decreased lid platform, and decreased UEH.
Blepharoptosis is a highly prevalent condition that we see every day in our clinics. You have the skillset to absolutely help your patients see and feel their very best.
Tips for Success: Ask, Look, then Look, and Ask! My favorite question: “Do you want your eyes to be more open?”
References
1 Vaca EE, Bricker JT, Helenowski I, Park ED, Alghoul MS. Identifying Aesthetically Appealing Upper Eyelid Topographic Proportions. Aesthetic Surgery Journal 2019, Vol 39(8) 824-834.
2 Knoll, Bianca et al. The Influence of Forehead, Brow, and Periorbital Aesthetics on Perceived Expression in the Youthful Face. American Society of Plastic Surgery. 2008.
3 Rhee, Seung et al. Biometric Study of Eyelid Shape and Dimensions of Different Races with References to Beauty. International Society of Plastic Surgery. 2012
4 Shen J et al. Optical Quality Assessment in Patients with Unilateral Congenital Ptosis: A Matched Case-Control Study. Hindawi Journal of Ophthalmology. 2020. Article ID 2653250: 1-9.
5 Seoung et al. Effects of upper lid blepharoplasty on visual quality in patients with lash ptosis and dermatochalasis. Int J Ophthalmol. 2016;9(9):1320-1324.