July 6, 2023
sponsored content
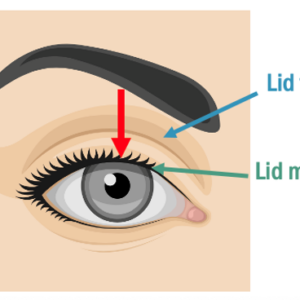
As practitioners we all see the natural changes that occur to the eye and eyelids due to aging. Over time, the superior eyelid margin vertical elevation tends to decrease.
One common condition I see in my practice is blepharoptosis, or what is often referred to as ptosis, which is a drooping of the upper eyelid that can affect one or both eyes. Age-related blepharoptosis is often caused by changes in the tone of Mueller’s muscle that is connected to the inferior portion of the elevator muscle. The Mueller’s muscle holds the tone of the eyelid, and as it becomes weaker, the vertical height of the lid reduces. Several things can affect eyelid position over time, including allergies, dry eye, or any other conditions that causes chronic lid rubbing. 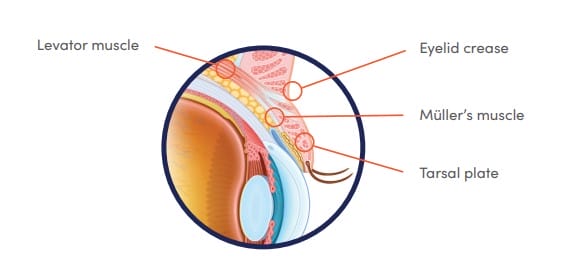
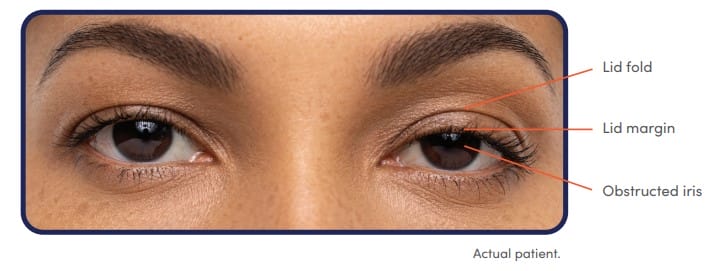
Anything that blocks the pupil can adversely affect vision. As such, ptosis can have a substantial effect on a patient’s visual outcome and thus their quality of life. It’s important that we as clinicians be cognizant that it’s not only the eyelid position that can potentially affect vision but also the trajectory of the eyelashes as they leave the lid margin. A person with mild ptosis but with an eyelash trajectory that encroaches into the line of sight will potentially have worse visual outcomes than a person who has a more moderate ptosis with eyelash trajectory that is away from the pupil and thus the line of sight.
Upneeq Expands Treatment Options
Until recently, we had only two options to treat patients with blepharoptosis. The first was to do nothing, and the second was to refer for surgery. Most patients would defer treatment and simply live with their blepharoptosis. However, in 2020, another option became available when the Food and Drug Administration approved RVL Pharmaceuticals’ Upneeq for the treatment of acquired blepharoptosis in adults. Upneeq is 0.1% oxymetazoline, which when instilled on the ocular surface, activates Mueller’s muscle to increase the height of the superior eyelid. Upneeq’s 0.1% oxymetazoline is a strong alpha-adrenergic agonist that has a five to one preference for alpha-2 adrenergic receptors over alpha-1 receptors. It is highly specific for alpha-2 receptors on the Mueller’s muscle. By activating the alpha-adrenergic receptors in Mueller’s muscle, Upneeq raises the ptotic eyelid by 1 to 1.3 mm (in two clinical trials).1
Clinically, I found it very interesting from the initial availability of Upneeq, that you could improve a patient’s eyelid position without surgery. Since it has been available, we’ve been using Upneeq as an option to treat our patients who have blepharoptosis. I discuss the pros and the cons of each treatment and its effects on cosmesis and vision. After all of the treatment options have been explained, the patient and I then consider what path is best for their specific needs.
What to Look for When Diagnosing Blepharoptosis
Some of the diagnostic technologies that we currently use in the office can help in screening for ptosis. Confocal scanning retinal imaging (CSRI) of the fundus is achieved when the inferior retina is imaged by light entering the superior pupil and the superior retina is imaged by light entering through the inferior people. When anything is blocking the superior pupil, such as a ptotic eyelid, it could appear as a shadow on the inferior portion of the CSRI. Just as ptosis affects the image acquisition of the retina, it can have a corresponding effect on the patient’s vision.
Identifying blepharoptosis is critical. I tend to pay attention to three things when I’m diagnosing patients with blepharoptosis. The first is assessing whether or not there is a dark region in the inferior portion of the CSRI image. If there is a dark area inferiorly, our technicians ask the patient whether they feel their eyelids ever get in the way of their vision.
The second thing I view is the visible vertical iris diameter. When we look at our patient, we expect to see most of the vertical iris diameter. Any hindrance of the view of the vertical iris indicates ptosis. I typically grade blepharoptosis as mild, moderate, or severe. The distance between the superior margin of the pupil and superior margin of the vertical iris diameter, is an important region to grade ptosis. For patients whose superior eyelid margin is between the superior 50% of the portion of the iris above the superior pupil margin, I consider it a mild blepharoptosis. For individuals whose eyelid margin is in between the superior pupil margin and below the 50 mark between the superior pupil and superior iris, I consider that a moderate ptosis. If the eyelid margin is within the pupil, I refer to that as a severe blepharoptosis.
The third component to consider when diagnosing ptosis is any type of asymmetry between the two eyes. An individual who has mild ptosis in both eyes will look much more symmetrical than those individuals who have a mild ptosis in one eye and normal eyelid position in the other eye. As such, asymmetries are inherently much easier for us to identify clinically because we’re used to detecting asymmetries in all the conditions that we assess with the eye.
Marginal Reflex Distance 1 (MRD-1) is the distance between the light reflex in the center of the pupil and the inferior margin of the superior eyelid. A normal MRD-1 is greater than 4 mm. This provides sufficient room between the superior lid margin and the pupil to provide adequate clearance of the eyelid margin from the pupil. A smaller MRD-1 equates to a more significant ptosis.
Blepharoptosis Versus Dermatochalasis
It is important to distinguish between blepharoptosis and dermatochalasis. Blepharoptosis describes a situation in which the lid margin is lower than we would physiologically expect it to be. Dermatochalasis is an excessive amount of loose skin on the superior lid that can fold over the lid margin. Upneeq is ideal for those individuals who have blepharoptosis. For people who have combined blepharoptosis and dermatochalasis, Upneeq will work, but the results may not be as easily seen as in those without dermatochalasis. The reason why that’s the case is that any lid lifting might be hidden by the excessive skin that’s overlying the lid margin in the presence of dermatochalasis.
Ptosis Can Cause Other Health Issues
Individuals can compensate for ptosis with alterations in head positioning. For instance, someone who has a ptosis that severely impairs their superior visual fields can develop a backward head tilt rather than rely on Mueller’s muscle to keep the lid out of the way of the pupil. Another example is a patient who may recruit the frontalis muscle in a compensatory manner in order to try to elevate the eyelids. This can cause potential headaches and eyestrain.
Additionally, contact lens wearers might also be adversely affected by ptosis. Multifocal contact lens wearers depend on simultaneously receiving both distance and near vision through the contact lens. As such, blocking a portion of the optical zone of the lens can have substantial effects to their visual outcomes.
How Upneeq Works
Patients typically have a positive response to Upneeq. The drop is created in a very comfortable vehicle that creates a comfortable instillation experience for most patients. Upneeq is a relatively fast-acting formula, and after the drops are applied to the eyes, results are seen as quickly as 10 minutes. If the drop is dosed in the office, most patients will see the benefits of the drop prior to leaving the office. Most patients comment that one drop will often correct the ptosis for most of the day.
One of the concerns we always have with chronically used eye drops is whether or not the individual will develop tachyphylaxis. Interestingly, there was no tachyphylaxis noted over the 42-day time period of the clinical trial. Following these individuals in my own office over the past several years has corroborated what was seen in the clinical trials. The efficacy of the drop maintains itself over time.
Unique Upneeq Distribution System
Upneeq is available as a prescription product and is distributed through RVL’s own pharmacy. However, depending on state laws, Upneeq can be retailed out of a practitioner’s office. In those instances, optometrists would have the ability to dispense the medication directly from your practice to the patient. When using the RVL pharmacy, a practitioner would simply go into their electronic prescribing system, select RVL as the pharmacy of choice, and prescribe the medication as they deem fit for the patient. The pharmacy then reaches out to the patient to discuss the cost of the drop and also to find out the supply that the patient would like to proceed with. Practitioners can prescribe it as a year supply, but the patient has flexibility with the supply that they order at any given time from the pharmacy. Upneeq is not covered by any major medical insurances, so it is an out-of-pocket cost for the patient.
To help increase awareness of the technology, we have an Upneeq poster in our pretest room. Sometimes patients will ask our technicians about it, and the technicians will be sure to make a note in the patient’s electronic health record so we know to discuss Upneeq with the patient in the exam room. We also have brochures in the exam room so that if patients aren’t aware that there’s a drop to improve eyelid position, they can see a brochure and ask about the product when we walk into the exam room. The brochures also provide us with educational information to give patients as well.
Patients Notice Additional Benefits
As we’ve had the opportunity to work with Upneeq, we’ve realized that it’s influence on vision is just as important as the potential cosmetic effects that it may have. The vision improvement is clinically very important, and we’ve seen firsthand the results and the perceptions that people experience when they utilize Upneeq. Patients with blepharoptosis who have been treated with Upneeq have also reported that their eyes don’t feel quite as tired, they don’t get headaches quite as much, and their vision has improved.
Now that Upneeq is available, it is much simpler to provide treatment for these patients. Understanding that we now have another option is a remarkable addition to our armamentarium of treatment options. Keeping this in mind and making sure that you’re offering this technology to appropriate patients is critical to ultimately optimizing your patients’ visual function.
Reference
1 Slonim CB, Foster S, Jaros M, et al. Association of oxymetazoline hydrochloride, 0.1%, solution administration with visual field in acquired ptosis: a pooled analysis of 2 randomized clinical trials. JAMA Ophthalmol. 2020;138(11):1168-1175.