April 11, 2023
There was recent excitement related to the possibility of scope expansion in California. The ability for California optometrists to perform selective laser trabeculoplasty (SLT) was within reach as legislative bills had passed the House and Senate during the 2022 session.
Unfortunately, the governor vetoed the legislation, but many feel it is inevitable that SLT will become part of optometry’s glaucoma treatment armamentarium. While optometrists have been able to perform SLT in several states going on 20 years, having a state as large as California would change the landscape dramatically.
Is SLT The Preferred Treatment?
SLT has flown under the radar as a glaucoma treatment for several reasons, including the difficulty device manufacturers have in competing with pharmaceutical companies in either advertising dollars or sales representatives. It took the Laser in Glaucoma and Ocular Hypertension Trial (LIGHT), with the results published in 2019,1 to make clinicians aware that SLT is an excellent (and perhaps preferred) initial therapy for ocular hypertension and mild to moderate open-angle glaucoma.2,3 Until then, SLT was viewed as an adjunctive treatment to medical therapy. The concept of using the laser to improve aqueous outflow was introduced in 1979 by Wise and Witter with application of the argon laser to the trabecular meshwork (TM) to create small burns.4 A 20-25% intraocular pressure (IOP) reduction was often obtained, though the effect was often temporary (lasting several years).4 IOP spikes, development of peripheral anterior synechiae, and acute anterior uveitis were reported adverse events with the mechanism for IOP lowering thought to be a mechanical contraction and opening of the trabeculum spaces.5
In 1995, Latina introduced SLT, using a 532 nm Q-switched, frequency-doubled Nd:YAG laser to apply marks to the TM, which caused minimal if any trabecular damage with the IOP-reducing mechanism thought to be a modification of trabecular health as compared to a mechanical opening.6 SLT lowered the IOP similar to argon laser trabeculoplasty (ALT), with fewer complications and over time became the preferred trabeculoplasty method.5 One limitation for both ALT and SLT is the IOP-lowering effect reduces over time, with SLT retreatment possible since little damage occurred.5,7
Can SLT Be a Substitute for Medication?
SLT meets the clinician’s wish list regarding what one wants from a glaucoma medication or modality. It lowers IOP effectively as well as being easy to administer, has few side effects, works with other medications or modalities, lowers IOP around the clock, and is cost effective.
Another advantage is that it removes the need for the patient to take their medication to reduce IOP. Adherence is no longer an issue, which is a problem with medications. Studies have shown that many glaucoma patients do not take their medications as directed, and IOP variability is one reason why glaucoma may progresss.8,9 Once SLT has been performed, IOP reduction will take place until therapy wanes as compared to patients needing to instill their eye drops daily. There are 24-hour IOP studies that have shown that SLT’s IOP-lowering effect lasts throughout the day and night.10 This compares to some medications such as beta blockers or alpha agonists that do not lower IOP over a 24-hour period (prostaglandins do work over a 24-hour period).11 Limitations to SLT usage include the cost of the laser and the technical skills required, such as the need to perform gonioscopy comfortably. As new medications are introduced, it may take several years before they are available on a patient’s formulary, while SLT reimbursement is usually covered by insurers.
New Developments with SLT
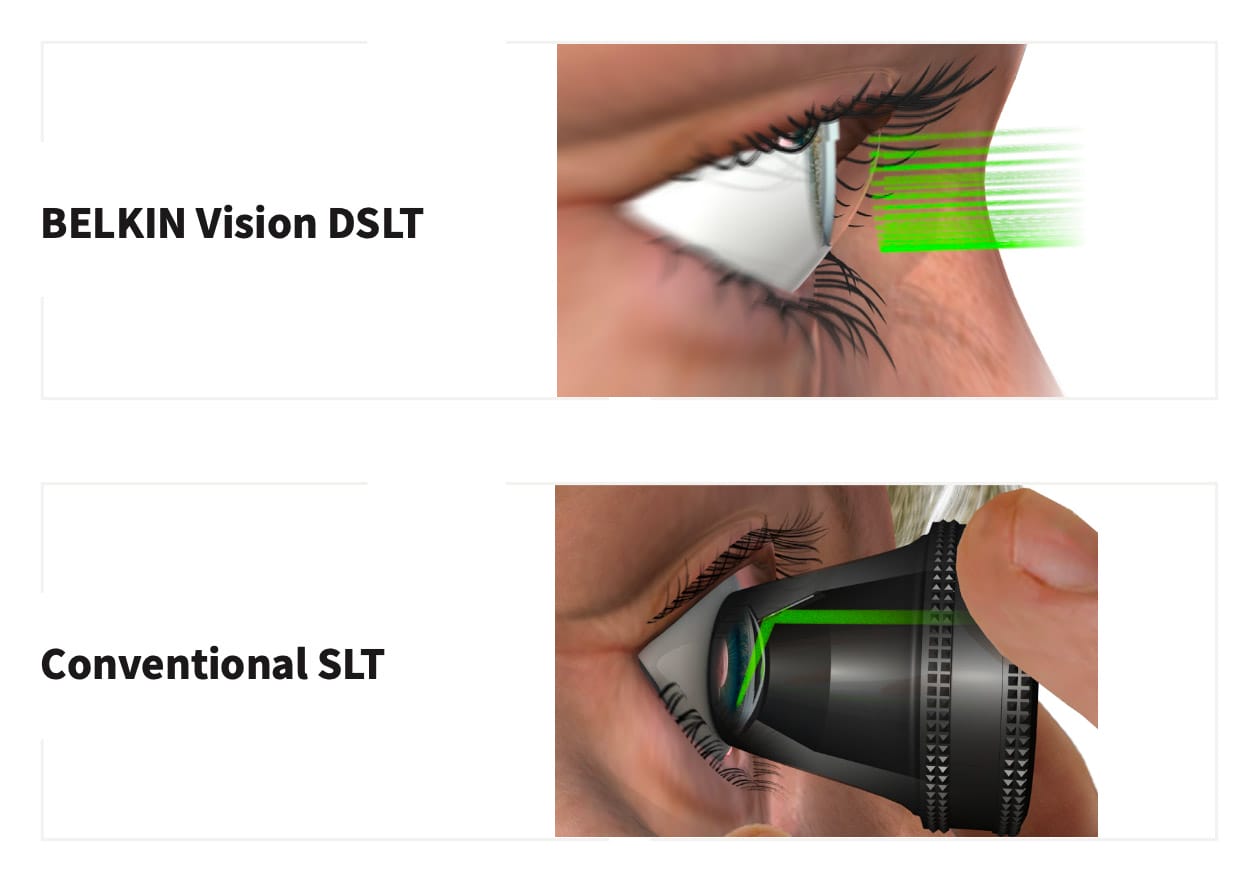
Several innovations are occurring within the laser space. First, Belkin Vision has developed the Eagle laser, which recently obtained a CE mark allowing its sale in Europe. This device performs direct selective laser trabeculoplasty (DSLT), which is an automated procedure done without the need of a goniolens.12,13,14 The procedure is fast, using image analysis and eye tracking to direct the laser through the sclera onto the trabeculum. It appears to be safe and effective in reducing IOP and is undergoing FDA clinical trials.
While DSLT’s original objective was to offer glaucoma therapy to countries having difficulty obtaining medications, it is understandable why this could be an important device for optometrists.14 Another development is the recently funded National Eye Institute clinical trial COAST (Clarifying the Optimal Application of SLT Therapy). Currently SLT is repeated when treatment fails and IOP rises. The COAST trial is a multicenter clinical trial examining the question of whether repeat low-energy laser applications, done on a yearly basis, allows the IOP-lowering effects to continue over time.15 The yearly laser touch-up is thought to keep the trabeculum invigorated, preventing IOP elevation. Thus, instead of a patient taking medication(s) daily, they have a yearly SLT treatment.
SLT has historically been the procedure clinicians turn to after medical therapy, when additional IOP lowering is needed. Due to its cost, safety, efficacy, and ease of application, SLT is becoming the preferred first-line glaucoma treatment. Both the American Academy of Ophthalmology and European Glaucoma Society recommend SLT as initial treatment for open-angle glaucoma, and an expected revision to the U.K.-based NICE guidelines should provide similar recommendations. The increased demand for SLT may make it difficult for ophthalmology to deliver to everyone in need, thus from a public health perspective, optometry’s use of SLT is understandable.
In a recent publication, doctors were asked whether the use of SLT by optometrists in the United Kingdom could improve health care outcomes within the National Health Service.16 The paper was positive, with the caveat that training is necessary but an improvement in health services is possible. A similar argument could be made in the United States as well as in other places around the world. Given the number of optometrists and their accessibility, one day SLT may be part of optometry’s scope of practice, not just in selected locations. This should improve the health of glaucoma patients worldwide.
References
1 Gazzard G, Konstantakopoulou E, Garway-Heath D, et al. Selective laser trabeculoplasty versus eye drops for first-line treatment of ocular hypertension and glaucoma (LIGHT): a multicentre randomized controlled trial. Lancet 2019;393:1505–16.
2 Garg A, Vickerstaff V, Nathwani N, et al. Primary selective laser trabeculoplasty for open-angle glaucoma and ocular hypertension. Clinical outcomes, predictors of success, and safety from the Laser in Glaucoma and Ocular Hypertension Trial. Ophthalmology 2019; 126:1238-1249.
3 Wright DM, Konstantakopoulou E, Montesan G, et al. Visual field outcomes from the multicenter, randomized controlled Laser in Glaucoma and Ocular Hypertension Trial (LIGHT). Ophthalmology 2020; 127:1313-1321.
4 Wise JB, Witter SL. Argon laser therapy for open-angle glaucoma. A pilot study. Arch Ophthalmol 1979;97:319–322.
5 Landers J. Selective laser trabeculoplasty: a review. Clin Experiment Ophthalmol 2021;49:1102-1110.
6 Garg A, Gazzard G. Selective laser trabeculoplasty: past, present, future. Eye 2018. 32:863-8676.
7 Realini T, Shillingford-Ricketts H, Burt D, et al. Long-term outcomes of selective laser trabeculoplasty for open-angle glaucoma in the Caribbean. Am J Ophthalmol 2021; 232 (12): 83-89.
8 Gatwood J, Brooks C, Meacham, et al. Facilitators and barriers to glaucoma medication adherence. J Glaucoma 2022; (1);31-36.
9 Nishida T, Moghimi S, Chang AC, et al. Association of intraocular pressure with retinal nerve fiber layer thinning in patients with glaucoma. JAMA Ophthalmol. Published online October 27, 2022.
10 Lee AC, Mosaed S, Weinreb RN, et al. Effect of laser trabeculoplasty on nocturnal intraocular pressure in medically treated glaucoma patients. Ophthalmology 2007; 114(4):666-670.
11 Liu JH, Medeiros FA, Slight JR, Weinreb RN. Comparing diurnal and nocturnal effects of brinzolamide and timolol on intraocular pressure in patients receiving latanoprost monotherapy. Ophthalmology 2009; 116(3):449-454.
12 Goldenfeld M, Belkin M, Dobkin-Bekman M, et al. Automated direct selective trabeculoplasty: first prospective clinical trial. Tran Vis Science & Technology 2021; 10 (3):5
13 Congdon N, Azuara-Blanco A, Solberg Y, et al. Direct selective laser trabeculoplasty in open angle glaucoma study design: a multicenter, randomized, controlled, investigator-masked trial (GLAUrious). Br J Ophthalmolool 2023;107:62-65.
14 Konstantakopoulou E, Gazzard G. Is selective laser trabeculoplasty shifting the glaucoma treatment paradigm in developing countries? Br J Ophthalmol; 2022;106:(9):1185-1186.
15 Realini T, Gazzard G, Latina M, Kass M. Low-energy selective laser trabeculoplasty repeated annually: rationale for the COAST Trial. J Glaucoma 2021; 30:545-551.
16 Konstantakopoulou E, Jones L, Nathwani, Gazzard G. Selective Laser Trabeculoplasty performed by optometrists – enablers and barriers to a shift in service delivery. Eye 2022 36:2006-2012.